Introduction: Septic shock is a complication of sepsis leading to circulatory and metabolic abnormalities. Cardiac ultrasound allows the assessment of vascular filling by measuring the diameter of the IVC (inferior vena cava) and detecting myocardial dysfunction. Objective: To assess the contribution of IVC ultrasound in the management of septic shock in children in the pediatric department of CHU-MEL. Methods: This was a prospective, descriptive, and analytical study conducted over a period of four months (February 2 to May 31, 2024). Results: The prevalence of septic shock was 4.9%. The most affected age group was infants under 12 months (62.5%). The most significant failures were renal (78.1%) and neurological (71.9%). The total amount of fluids administered with vascular filling monitoring by IVC ultrasound varied from 0 to 65ml/kg. It was adapted to each child based on IVC dilation. The vasoactive drug of choice was norepinephrine. Shock resolution was achieved in 31.3%. The mortality rate was 84.4%.Conclusion: IVC ultrasound helped avoid both hypovolemia and harmful excessive fluid administration by adapting the amount of fluids to each child based on their IVC diameter. Adequate training in bedside echocardiography would allow pediatricians to improve the hemodynamic management of septic shock in children.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Septic shock is a public health issue worldwide, especially in developing countries. In 2017, there were 48.9 million cases of septic shock globally, with 11 million deaths
[1]
Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study. The Lancet. 2020; 395(10219): 200-211.
[1]
. Nearly half of these cases involved children under five years old. Additionally, 2.9 million of the recorded deaths were among these children
[1]
Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study. The Lancet. 2020; 395(10219): 200-211.
[1]
. The management of septic shock is based on two pillars: infection control and hemodynamic stabilization. Crystalloids are the fluid of choice for hemodynamic stabilization, and norepinephrine is the first-line vasopressor in case of fluid resuscitation failure
[2]
Young Ran Lee, Pharm D, Taryn B, et al. Sepsis management. CCSAP. 2019.
[2]
. Vascular filling must neither be insufficient nor cause harmful fluid overload. In this respect, cardiac ultrasound allows the assessment of vascular filling by measuring the IVC diameter and simultaneously detecting potential myocardial dysfunction. In a 2013 Indian study, cases of non-response to fluid resuscitation associated with vasopressors were related to insufficient filling or myocardial dysfunction
[3]
Ranjit S, Kissoon N. Bedside echocardiography is useful in assessing children with fluid and inotrope resistant septic shock. Indian J Crit Care Med. 2013; 17(4): 224‑30.
[3]
. Cardiac ultrasound also helps avoid excessive filling that could lead from vasoplegia to acute pulmonary edema
[4]
Kaiser RS, Sarkar M, Raut SK, et al. A Study to Compare Ultrasound-guided and Clinically Guided Fluid Management in Children with Septic Shock. Indian J Crit Care Med. 2023; 27(2): 139‑46.
[4]
.
The objective of this study was to assess the contribution of IVC ultrasound in vascular filling during the management of septic shock in children in the pediatric department of CHU-MEL in 2024.
2. Patients and Methods
This was a prospective, descriptive, and analytical study conducted over a period of four months from February 2, 2024, to May 31, 2024. It included children admitted to the pediatric department of CHU-MEL who were diagnosed with septic shock during the study period. Sepsis was defined as arterial hypotension requiring vasopressors to maintain a mean arterial pressure (MAP) of 65 mmHg or higher, a blood lactate level above 2 mmol/liter, and a SOFA score above 2. The patients were aged from one month to 17 years old. IVC ultrasound was performed before any fluid resuscitation and adrenaline administration and also after vascular filling. Filling was done in the presence of a collapsed IVC and repeated until a normal diameter was achieved. The fluid used for resuscitation was isotonic saline for well-nourished children and a DARROW equivalent (a solution comprising equal parts of saline and 5% glucose) for severely malnourished children. The amount of fluid administered varied from 10 to 20 ml/kg per resuscitation and was adapted to each child based on the IVC dilation measured by ultrasound.
Norepinephrine was only administered in the persistence of shock signs after normalizing blood volume (normal IVC diameter on ultrasound). It was initiated immediately upon detecting cardiac failure on ultrasound. Data were analyzed using Epi Info version 7.2.5.0 and Excel 2013 software. Proportions were compared using the chi-square test, and a p-value below 0.05 was considered significant.
3. Results
During the study period, 774 children were admitted; the prevalence of sepsis was 9.9% (n=77), and septic shock was 4.9% (n=38). Only 32 children were included in the study. Non-performance of IVC ultrasound (n=4) and administration of adrenaline before ultrasound (n=2) were reasons for non-inclusion.
The average age was nine months, ranging from four to 48 months. The most represented age group was infants under one year. Females predominated with a sex ratio of 0.68.
All children had cold extremities and imperceptible pulses, and 78.1% had prolonged capillary refill time (n=25). Before the first resuscitation, 68.8% had arterial hypotension (n=22). After the first resuscitation, arterial hypotension was observed in 75% of children (n=24) and persisted after the second resuscitation.
The most common organ failures were renal (78.1%), neurological (71.9%), cardiovascular (9.4%), hematological (6.1%), and hepatic (3.1%).
Infection sources were distributed as follows: 96.9% pulmonary, 75% meningeal, 50% digestive, 37.1% cutaneous, and 3.1% urinary as well as ENT.
Coma was associated with septic shock in 71.9% of children (n=23). No child had jaundice, but 28.1% had hepatomegaly (n=9), and 18.8% experienced bleeding (n=6).
Bacteriologically, 24 blood cultures were effectively collected and processed. Nine cultures were contributive out of the 24 performed. The identified pathogens were Staphylococcus aureus (n=3), Burkholderia cepacia (n=2), Streptococcus pneumoniae (n=1), Serratia marcescens (n=1), Pseudomonas aeruginosa (n=1), and Acinetobacter sp (n=1).
A total of 31 children received fluid resuscitation.
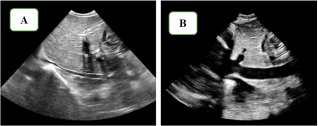
Figure 1. IVC Ultrasound Image (collapsed in A and plethoric in B).
The IVC was collapsed in 31 out of the 32 included children, as shown in image A of Figure 1. At the end of the first resuscitation, four children (12.5%) had regained a normal IVC diameter (Figure 1), 25 required a second resuscitation, and two required three resuscitations.
All children received a vasoactive drug, specifically norepinephrine. One child also received dobutamine for associated cardiogenic shock.
Follow-ups were challenging, with facial swelling without signs of acute pulmonary edema (n=3) and oliguria (n=5).
Shock resolution was effective in ten children, and favorable outcomes were observed in five. The mortality rate was 84.4% (n=27).
4. Discussion
The prevalence of septic shock in this study was 4.9%. This result is similar to that found in 2019 in the intensive care unit of CNHU
[5]
Akodjenou J, Mewanou S, Ahounou E et al. Fréquence et prise en charge du choc septique en réanimation dans un pays à ressources limitées : cas du Centre National Hospitalier et Universitaire Hubert Koutoukou Maga (CNHU-HKM) de Cotonou. Journal de la Société Biologie Clinique Benin. 2021; 37: 41‑48.
[5]
. Although their study involved an adult population, the prevalence of septic shock was 4.7%. This incidence is twice as high as that found in Mali in 2018 in a pediatric population (2.4% frequency)
[6]
Manu KN. Choc septique en réanimation du CHU Gabriel Touré de Médecine et d’OdontoStomatologie. 2015: 83 p.
[6]
. This could be explained by the increasing incidence of septic shock described in the literature
[7]
Munoz M. Choc septique : incidence, mortalité et taux de réhospitalisation dans les réanimations Françaises, une étude de cohorte nationale. 2021: 32p.
[7]
.
The average age of the children was nine months, with the most affected age group being infants under one year old (62.5%). This result is similar to the one found in 2018 at CHU Gabriel TOURE in Mali in children aged one month to 15 years; the most affected age group was infants under two years old (53.49%)
[6]
Manu KN. Choc septique en réanimation du CHU Gabriel Touré de Médecine et d’OdontoStomatologie. 2015: 83 p.
[6]
. The observed variation could be explained by the fact that their study did not distinguish the age group from one to two years (grouped as one month to two years), unlike the present study which segmented it into two distinct groups: one month to one year, and one to two years
[6]
Manu KN. Choc septique en réanimation du CHU Gabriel Touré de Médecine et d’OdontoStomatologie. 2015: 83 p.
[6]
. This result is consistent with literature data which estimate that the incidence is highest among infants
[8]
Watson RS, Carcillo JA, Linde-Zwirble WT, et al. The epidemiology of severe sepsis in children in the United States. Am J Respir Crit Care Med. 2003; 167(5): 695‑701.
[8]
.
The study population was predominantly female with a sex ratio of 0.68. This result is also similar to that of the Malian team with 74% girls
[6]
Manu KN. Choc septique en réanimation du CHU Gabriel Touré de Médecine et d’OdontoStomatologie. 2015: 83 p.
[6]
.
All the children had cold extremities with an imperceptible pulse and 78% had prolonged capillary refill time. Before the first resuscitation, 68.8% had arterial hypotension. After the first and second resuscitations, the proportion of arterial hypotension was 75%. This result is consistent with literature data showing that, unlike in adults, hypotension is not necessary for the diagnosis of septic shock in children, as it is a late sign indicative of shock decompensation
[9]
Vergnaud E, Sylvestre JB, Orliaguet G. Choc septique chez l’enfant. Anesth Réanimation. 2022; 8(5): 506‑11.
[9]
.
In this study, the infection foci found were in order of frequency: pulmonary (96.9%), meningeal and digestive (50%), cutaneous (37.1%), urinary (3.1%), and ENT (3.1%). A Colombian study also found a predominance of respiratory foci in 2012
[10]
Ortíz G, Dueñas C, Rodríguez F. Épidémiologie de la septicémie dans les unités de soins intensifs colombiennes. Biomedica. 2014; 34(1): 40-7.
[10]
. This predominance was similar to that previously found in the department in 2022
[11]
Dossou Togbe L. Aspects épidémiologiques, diagnostiques, thérapeutiques et évolutifs du sepsis dans le service de pédiatrie du centre hospitalier et universitaire de la mère et de l’enfant lagune (CHUMEL) [Mémoire de DES de pédiatrie. Cotonou: Faculté des sciences de la santé; 2022.
[11]
. However, osteoarticular (48.8%) and cutaneous (23.2%) foci were the most common in the Malian study; the observed differences could be due to the fact that their study populations included all cases of sepsis, whereas here, only septic shock was considered
[6]
Manu KN. Choc septique en réanimation du CHU Gabriel Touré de Médecine et d’OdontoStomatologie. 2015: 83 p.
[6]
.
In the first ultrasound, all children except one had a collapsed IVC. This frequency of fluid deficit requiring fluid resuscitation in children with septic shock was noted in India in 2023
[3]
Ranjit S, Kissoon N. Bedside echocardiography is useful in assessing children with fluid and inotrope resistant septic shock. Indian J Crit Care Med. 2013; 17(4): 224‑30.
[3]
. This hypovolemia was clinically apparent in only 9.3% of children. Thus, IVC ultrasound allowed us to distinguish children with hypovolemia (96.8%) from those who did not need vascular filling (3.2%). The ultrasound enabled the recognition of hypovolemia associated with septic shock, early initiation of vasoactive drugs if needed, and avoidance of vascular overload.
Only 12.5% of the children needed a single resuscitation, 78.1% needed a second resuscitation, and 6.3% needed a third resuscitation. The average amount of fluid received was 40ml/kg, ranging from 0 to 65ml/kg. Similar results were found in the literature with fluid boluses between 30 and 50ml/kg in a population of children whose first ultrasound was performed after the first resuscitation
[4]
Kaiser RS, Sarkar M, Raut SK, et al. A Study to Compare Ultrasound-guided and Clinically Guided Fluid Management in Children with Septic Shock. Indian J Crit Care Med. 2023; 27(2): 139‑46.
[4]
. However, in a more recent study in India, a larger proportion of children needed more than 60 ml/kg of fluid boluses; indeed, there was shock resistance in 49.5% of children who received 60ml/kg of fluid in the first hour. The most frequent result of the echocardiography performed after 60ml/kg was uncorrected hypovolemia evidenced by IVC collapse in 12 out of 22 patients
[3]
Ranjit S, Kissoon N. Bedside echocardiography is useful in assessing children with fluid and inotrope resistant septic shock. Indian J Crit Care Med. 2013; 17(4): 224‑30.
[3]
. This higher number is probably due to the fact that they only included children who had received at least 60ml/kg of fluids in their study. Thus, IVC ultrasound enabled decision-making on whether to continue or stop vascular filling. Each child received the necessary amount of fluids to correct their hypovolemia. IVC ultrasound allows the early initiation of vasoactive drugs as soon as the fluid deficit is corrected.
Signs of overload, such as palpebral edema and/or facial swelling, developed during the course of 9.7% of the study population, as also found in the literature
[4]
Kaiser RS, Sarkar M, Raut SK, et al. A Study to Compare Ultrasound-guided and Clinically Guided Fluid Management in Children with Septic Shock. Indian J Crit Care Med. 2023; 27(2): 139‑46.
[4]
. Renal failure with oliguria associated with these conditions and the additional amount of fluids received in the context of blood product administration could explain this outcome. There was no significant association between the occurrence of overload signs and the total amount of fluids received. However, the mortality rate was very high, as found in other local studies
[5]
Akodjenou J, Mewanou S, Ahounou E et al. Fréquence et prise en charge du choc septique en réanimation dans un pays à ressources limitées : cas du Centre National Hospitalier et Universitaire Hubert Koutoukou Maga (CNHU-HKM) de Cotonou. Journal de la Société Biologie Clinique Benin. 2021; 37: 41‑48.
[11]
Dossou Togbe L. Aspects épidémiologiques, diagnostiques, thérapeutiques et évolutifs du sepsis dans le service de pédiatrie du centre hospitalier et universitaire de la mère et de l’enfant lagune (CHUMEL) [Mémoire de DES de pédiatrie. Cotonou: Faculté des sciences de la santé; 2022.
[5, 11]
.
5. Conclusion
From a hemodynamic perspective, IVC ultrasound enabled us to diagnose non-apparent hypovolemia associated with septic shock in children, avoid excessive fluid resuscitation by adapting the amount of fluids to each child based on their IVC diameter, verify the effectiveness of vascular filling at the end of resuscitation, and initiate vasoactive drugs as soon as vascular filling effectiveness was achieved.
Adequate training in bedside echocardiography would enable pediatricians to improve the management of septic shock in children.
Abbreviations
CHU
Hospital and University Center
CHU-MEL
Child Hospital and University Center - Lagune
Acknowledgments
The authors wish to thank Njitam Gassam Stéphane Brice for his contributions to the translation of this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest regarding the publication of this paper.
References
[1]
Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study. The Lancet. 2020; 395(10219): 200-211.
[2]
Young Ran Lee, Pharm D, Taryn B, et al. Sepsis management. CCSAP. 2019.
[3]
Ranjit S, Kissoon N. Bedside echocardiography is useful in assessing children with fluid and inotrope resistant septic shock. Indian J Crit Care Med. 2013; 17(4): 224‑30.
[4]
Kaiser RS, Sarkar M, Raut SK, et al. A Study to Compare Ultrasound-guided and Clinically Guided Fluid Management in Children with Septic Shock. Indian J Crit Care Med. 2023; 27(2): 139‑46.
[5]
Akodjenou J, Mewanou S, Ahounou E et al. Fréquence et prise en charge du choc septique en réanimation dans un pays à ressources limitées : cas du Centre National Hospitalier et Universitaire Hubert Koutoukou Maga (CNHU-HKM) de Cotonou. Journal de la Société Biologie Clinique Benin. 2021; 37: 41‑48.
[6]
Manu KN. Choc septique en réanimation du CHU Gabriel Touré de Médecine et d’OdontoStomatologie. 2015: 83 p.
[7]
Munoz M. Choc septique : incidence, mortalité et taux de réhospitalisation dans les réanimations Françaises, une étude de cohorte nationale. 2021: 32p.
[8]
Watson RS, Carcillo JA, Linde-Zwirble WT, et al. The epidemiology of severe sepsis in children in the United States. Am J Respir Crit Care Med. 2003; 167(5): 695‑701.
[9]
Vergnaud E, Sylvestre JB, Orliaguet G. Choc septique chez l’enfant. Anesth Réanimation. 2022; 8(5): 506‑11.
[10]
Ortíz G, Dueñas C, Rodríguez F. Épidémiologie de la septicémie dans les unités de soins intensifs colombiennes. Biomedica. 2014; 34(1): 40-7.
[11]
Dossou Togbe L. Aspects épidémiologiques, diagnostiques, thérapeutiques et évolutifs du sepsis dans le service de pédiatrie du centre hospitalier et universitaire de la mère et de l’enfant lagune (CHUMEL) [Mémoire de DES de pédiatrie. Cotonou: Faculté des sciences de la santé; 2022.
Joseph, A., Annatou, Y., Carine, D., Jules, A., Eugène, Z. (2025). Contribution of Inferior Vena Cava Ultrasound Monitoring in the Management of Septic Shock in Children at the CHU-MEL. American Journal of Pediatrics, 11(1), 26-29. https://doi.org/10.11648/j.ajp.20251101.14
Joseph, A.; Annatou, Y.; Carine, D.; Jules, A.; Eugène, Z. Contribution of Inferior Vena Cava Ultrasound Monitoring in the Management of Septic Shock in Children at the CHU-MEL. Am. J. Pediatr.2025, 11(1), 26-29. doi: 10.11648/j.ajp.20251101.14
Joseph A, Annatou Y, Carine D, Jules A, Eugène Z. Contribution of Inferior Vena Cava Ultrasound Monitoring in the Management of Septic Shock in Children at the CHU-MEL. Am J Pediatr. 2025;11(1):26-29. doi: 10.11648/j.ajp.20251101.14
@article{10.11648/j.ajp.20251101.14,
author = {Akodjenou Joseph and Yakoubou Annatou and Dadjo Carine and Alao Jules and Zoumenou Eugène},
title = {Contribution of Inferior Vena Cava Ultrasound Monitoring in the Management of Septic Shock in Children at the CHU-MEL
},
journal = {American Journal of Pediatrics},
volume = {11},
number = {1},
pages = {26-29},
doi = {10.11648/j.ajp.20251101.14},
url = {https://doi.org/10.11648/j.ajp.20251101.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20251101.14},
abstract = {Introduction: Septic shock is a complication of sepsis leading to circulatory and metabolic abnormalities. Cardiac ultrasound allows the assessment of vascular filling by measuring the diameter of the IVC (inferior vena cava) and detecting myocardial dysfunction. Objective: To assess the contribution of IVC ultrasound in the management of septic shock in children in the pediatric department of CHU-MEL. Methods: This was a prospective, descriptive, and analytical study conducted over a period of four months (February 2 to May 31, 2024). Results: The prevalence of septic shock was 4.9%. The most affected age group was infants under 12 months (62.5%). The most significant failures were renal (78.1%) and neurological (71.9%). The total amount of fluids administered with vascular filling monitoring by IVC ultrasound varied from 0 to 65ml/kg. It was adapted to each child based on IVC dilation. The vasoactive drug of choice was norepinephrine. Shock resolution was achieved in 31.3%. The mortality rate was 84.4%. Conclusion: IVC ultrasound helped avoid both hypovolemia and harmful excessive fluid administration by adapting the amount of fluids to each child based on their IVC diameter. Adequate training in bedside echocardiography would allow pediatricians to improve the hemodynamic management of septic shock in children.
},
year = {2025}
}
TY - JOUR
T1 - Contribution of Inferior Vena Cava Ultrasound Monitoring in the Management of Septic Shock in Children at the CHU-MEL
AU - Akodjenou Joseph
AU - Yakoubou Annatou
AU - Dadjo Carine
AU - Alao Jules
AU - Zoumenou Eugène
Y1 - 2025/02/26
PY - 2025
N1 - https://doi.org/10.11648/j.ajp.20251101.14
DO - 10.11648/j.ajp.20251101.14
T2 - American Journal of Pediatrics
JF - American Journal of Pediatrics
JO - American Journal of Pediatrics
SP - 26
EP - 29
PB - Science Publishing Group
SN - 2472-0909
UR - https://doi.org/10.11648/j.ajp.20251101.14
AB - Introduction: Septic shock is a complication of sepsis leading to circulatory and metabolic abnormalities. Cardiac ultrasound allows the assessment of vascular filling by measuring the diameter of the IVC (inferior vena cava) and detecting myocardial dysfunction. Objective: To assess the contribution of IVC ultrasound in the management of septic shock in children in the pediatric department of CHU-MEL. Methods: This was a prospective, descriptive, and analytical study conducted over a period of four months (February 2 to May 31, 2024). Results: The prevalence of septic shock was 4.9%. The most affected age group was infants under 12 months (62.5%). The most significant failures were renal (78.1%) and neurological (71.9%). The total amount of fluids administered with vascular filling monitoring by IVC ultrasound varied from 0 to 65ml/kg. It was adapted to each child based on IVC dilation. The vasoactive drug of choice was norepinephrine. Shock resolution was achieved in 31.3%. The mortality rate was 84.4%. Conclusion: IVC ultrasound helped avoid both hypovolemia and harmful excessive fluid administration by adapting the amount of fluids to each child based on their IVC diameter. Adequate training in bedside echocardiography would allow pediatricians to improve the hemodynamic management of septic shock in children.
VL - 11
IS - 1
ER -
Joseph, A., Annatou, Y., Carine, D., Jules, A., Eugène, Z. (2025). Contribution of Inferior Vena Cava Ultrasound Monitoring in the Management of Septic Shock in Children at the CHU-MEL. American Journal of Pediatrics, 11(1), 26-29. https://doi.org/10.11648/j.ajp.20251101.14
Joseph, A.; Annatou, Y.; Carine, D.; Jules, A.; Eugène, Z. Contribution of Inferior Vena Cava Ultrasound Monitoring in the Management of Septic Shock in Children at the CHU-MEL. Am. J. Pediatr.2025, 11(1), 26-29. doi: 10.11648/j.ajp.20251101.14
Joseph A, Annatou Y, Carine D, Jules A, Eugène Z. Contribution of Inferior Vena Cava Ultrasound Monitoring in the Management of Septic Shock in Children at the CHU-MEL. Am J Pediatr. 2025;11(1):26-29. doi: 10.11648/j.ajp.20251101.14
@article{10.11648/j.ajp.20251101.14,
author = {Akodjenou Joseph and Yakoubou Annatou and Dadjo Carine and Alao Jules and Zoumenou Eugène},
title = {Contribution of Inferior Vena Cava Ultrasound Monitoring in the Management of Septic Shock in Children at the CHU-MEL
},
journal = {American Journal of Pediatrics},
volume = {11},
number = {1},
pages = {26-29},
doi = {10.11648/j.ajp.20251101.14},
url = {https://doi.org/10.11648/j.ajp.20251101.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20251101.14},
abstract = {Introduction: Septic shock is a complication of sepsis leading to circulatory and metabolic abnormalities. Cardiac ultrasound allows the assessment of vascular filling by measuring the diameter of the IVC (inferior vena cava) and detecting myocardial dysfunction. Objective: To assess the contribution of IVC ultrasound in the management of septic shock in children in the pediatric department of CHU-MEL. Methods: This was a prospective, descriptive, and analytical study conducted over a period of four months (February 2 to May 31, 2024). Results: The prevalence of septic shock was 4.9%. The most affected age group was infants under 12 months (62.5%). The most significant failures were renal (78.1%) and neurological (71.9%). The total amount of fluids administered with vascular filling monitoring by IVC ultrasound varied from 0 to 65ml/kg. It was adapted to each child based on IVC dilation. The vasoactive drug of choice was norepinephrine. Shock resolution was achieved in 31.3%. The mortality rate was 84.4%. Conclusion: IVC ultrasound helped avoid both hypovolemia and harmful excessive fluid administration by adapting the amount of fluids to each child based on their IVC diameter. Adequate training in bedside echocardiography would allow pediatricians to improve the hemodynamic management of septic shock in children.
},
year = {2025}
}
TY - JOUR
T1 - Contribution of Inferior Vena Cava Ultrasound Monitoring in the Management of Septic Shock in Children at the CHU-MEL
AU - Akodjenou Joseph
AU - Yakoubou Annatou
AU - Dadjo Carine
AU - Alao Jules
AU - Zoumenou Eugène
Y1 - 2025/02/26
PY - 2025
N1 - https://doi.org/10.11648/j.ajp.20251101.14
DO - 10.11648/j.ajp.20251101.14
T2 - American Journal of Pediatrics
JF - American Journal of Pediatrics
JO - American Journal of Pediatrics
SP - 26
EP - 29
PB - Science Publishing Group
SN - 2472-0909
UR - https://doi.org/10.11648/j.ajp.20251101.14
AB - Introduction: Septic shock is a complication of sepsis leading to circulatory and metabolic abnormalities. Cardiac ultrasound allows the assessment of vascular filling by measuring the diameter of the IVC (inferior vena cava) and detecting myocardial dysfunction. Objective: To assess the contribution of IVC ultrasound in the management of septic shock in children in the pediatric department of CHU-MEL. Methods: This was a prospective, descriptive, and analytical study conducted over a period of four months (February 2 to May 31, 2024). Results: The prevalence of septic shock was 4.9%. The most affected age group was infants under 12 months (62.5%). The most significant failures were renal (78.1%) and neurological (71.9%). The total amount of fluids administered with vascular filling monitoring by IVC ultrasound varied from 0 to 65ml/kg. It was adapted to each child based on IVC dilation. The vasoactive drug of choice was norepinephrine. Shock resolution was achieved in 31.3%. The mortality rate was 84.4%. Conclusion: IVC ultrasound helped avoid both hypovolemia and harmful excessive fluid administration by adapting the amount of fluids to each child based on their IVC diameter. Adequate training in bedside echocardiography would allow pediatricians to improve the hemodynamic management of septic shock in children.
VL - 11
IS - 1
ER -