Background: Down syndrome (DS) or trisomy 21 is a genetic disorder caused by unusual cell division and an extra copy of chromosome 21. DS is characterized by phenotypic characteristics identified clinically and is the most common genetic cause of intellectual disability in children. DS can also result in other medical complications that involve the heart, the digestive system and memory disabilities leading to Alzheimer’s disease (AD). Although diagnosis is made clinically, screening tests such as chorionic villus sampling (CVS), amniocentesis and ultrasound detecting translucency of the nuchal folds of the neck are used to detect it at its early stages. There is no known treatment for DS, however, early detection and intervention can improve quality of life (QoL) for patients and their parents. Aims: This review aims to identify the importance of neuroimaging, particularly magnetic resonance imaging (MRI), in early diagnosis of DS. The review will explore how neuroanatomical changes can guide future research and focus interventions to target needs of individuals. Method: This review included 12 studies on DS from the year 2000 to date. Participants included ranged from fetus to 15-year-old teenagers. Diagnosis of DS was first made by CVS, amniocentesis or ultrasound depending on mother’s preference followed by karyotyping confirming trisomy 21. The main imaging modality included in the review is high-resolution MRI which all participants underwent for comparison. Results: Results of the MRI showed an overall reduction in volume in different areas of the brain in DS patients compared to controls. Most prominent volume reduction were found in the frontal lobes, hippocampus and brainstem. With increasing age there was preservation of volumes in parietal and temporal lobes. After the age of 11 years, changes in the grey and white matters started to appear. Conclusion: Early detection of brain changes, especially in fetus, could improve developmental outcomes for people suffering from DS by providing early and tailored interventions focusing on potential cognitive impairments associated to damaged brain areas. These neuroanatomical changes in DS patients are correlated to cognitive disabilities that are controlled by specific areas of the brain, relating this review to its clinical relevance. Some limitations of the studies included in the review was the small sample size. Selection bias was introduced by recruiting participants solely from hospitals where healthcare access might be limited to those can afford it. Some strengths include the consistency in diagnosing DS first with chorionic villus sampling, amniocentesis and ultrasound and confirmation it with karyotyping.
| Published in | American Journal of Pediatrics (Volume 11, Issue 2) |
| DOI | 10.11648/j.ajp.20251102.18 |
| Page(s) | 81-92 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Down Syndrome, Trisomy 21, Developing Fetus, Childhood, Magnetic Resonance Imaging, MRI, Cognitive Disabilities
Study | Age | Total number of participants | MRI sequence (T1 or T2-weighted image) | Power of the magnetic field measured in Tesla (T) | Results |
|---|---|---|---|---|---|
(Patkee et al., 2020) | 21-46 weeks gestation | 124 | T2- weighted image | 1.5T 3.0T | Reduced cerebellar volume in 2nd trimester Alteration in cortical growth in 3rd trimester |
(Kitano et al., 2023) | 22-37 weeks gestation | 22 | T2- weighted image | 1.5T | Small cerebellar vermis Large fourth ventricle Small cerebellar:fourth ventricle ratio |
(Tarui et al., 2019) | 25-29 weeks gestation | 21 | T2- weighted image | 1.5T | Decreased cortical volume growth Decreased subcortical parenchymal volume Decreased cerebellar hemispheric volumes |
(Yun et al., 2020) | 29 weeks gestation | 26 | T2- weighted image | 1.5T | Decrease sulcal depth in bilateral Sylvian fissures, right central and parieto-occipital sulci Increased sulcal depth in left superior temporal sulcus |
(Fujii et al., 2017) | 0-11 years | 64 | T1- weighted image T2- weighted image | 1.5T 3.0T | Smaller ventral pons |
(Gunbey et al., 2016) | 2 years | 18 | T1- weighted image | 1.5T | Reduced grey matter volumes of left putamen, thalamus, caudate nucleus, cerebellar cortex, brainstem and corpus callosum Reduced subcortical grey matter and total cortical grey matter of both hemispheres Decreased volume of right cerebellar white matter |
(Shiohama et al., 2019) | < 3 years | 40 | T1- weighted image | 3.0T | Decreased brain volumes in the grey and white matter, brainstem and cortical areas of the brain |
(Śmigielska-Kuzia et al., 2011) | 6 years 8 years | 49 | T1- weighted image T2- weighted image | 1.5T | Reduction in total brain volumes, frontal lobe and temporal lobe volumes Reudction in volumes of the hippocampus and amygdala |
(Carducci et al., 2013) | 10 years | 48 | T1- weighted image | 1.5T | Reduction in total brain volume Reduction in grey matter of frontal lobes, white matter of frontal and parietal lobes and brainstem Preservation of grey matter of parietal and temporal lobes and white matter of temporal lobe |
(Pinter et al., 2001) | 11 years | 31 | T1- weighted image | 1.5T | Smaller overall brain volume Small cerebellar volume that is disproportional to larger subcortical grey matter volume Preservation of parietal lobe grey matter Preservation of temporal lobe white matter |
(Hamadelseed & Skutella, 2023) | 14-15 years | 25 | T1- weighted image | 1.5T 3.0T | Mean total brain volume 20% smaller than the control group No difference in parietal lobe, dentate gyrus, fusiform gyrus and parahippocampal gyrus |
(Menghini et al., 2011) | 15 years | 24 | T1- weighted image | 1.5T | Reduced total brain volumes (TBV), grey matter volume (GMV) and white matter (WMV) volume |
Region | Calculated volumes in cubic cm | |
|---|---|---|
Down syndrome | Controls | |
Grey matter (GM) | 677.3 cm3 | 783.6 cm3 |
White matter (WM) | 373.8 cm3 | 441.2 cm3 |
Total brain volume (TBV) | 1443.6 cm3 | 1628.7 cm3 |
DS | Down Syndrome |
AD | Alzheimer’s Disease |
CVS | Chorionic Villus Sampling |
QoL | Quality of Life |
MRI | Magnetic Resonance Imaging |
BHCG | Beta Human Chorionic Gonadotropin |
IQ | Intelligence Quotient |
TBSS | Stanford Binet Intelligence Scale |
WISC-R | Revised Wechsler Intelligence Scale for Children |
DWI | Diffusion Weighted Imaging |
T unit | Teslas Unit of Measurement |
CH | Chloral Hydrate |
TBV | Total Brain Volume |
GMV | Grey Matter Volume |
WMV | White Matter Volume |
HV | Height Volume |
APDV | Anteroposterior Diameter Volume |
OFD | Occipitofrontal Diameter |
HC | Head Circumference |
STC | Superior Temporal Cortex |
ACC | Anterior Cingulate Cortex |
MFC | Middle frontal Cortex |
CHF | Congestive Heart Failure |
PET | Positron Emission Tomography |
Study | Ethical guidlines |
|---|---|
(Patkee et al., 2020) | West London and GTAC Research Ethics Committee (REC) for DS participants and fetal controls and the Dulwich NREC for neonatal controls |
(Kitano et al., 2023) | Approved by the Institutional Review Board (protocol #10214) |
(Tarui et al., 2019) | The study was approved by the Institutional Review Boards of Tufts Medical Center (TMC) and Boston Children’s Hospital (BCH) |
(Yun et al., 2020) | Institutional review boards of participating institutions at Boston Children’s Hospital (BCH) and Tufts Medical Center (TMC) |
(Fujii et al., 2017) | The hospital’s research ethics board |
(Gunbey et al., 2016) | Ethics Committee of Ondokuz Mayıs University Medical School, Samsun, Turkey |
(Shiohama et al., 2019) | Institutional Review Board at Boston Children Hospital (BCH) |
(Śmigielska-Kuzia et al., 2011) | Ethical Committee at the Medical University of Bialystok, Poland |
(Carducci et al., 2013) | Institutional review board approval |
(Pinter et al., 2001) | Not mentioned |
(Hamadelseed & Skutella, 2023) | Not mentioned |
(Menghini et al., 2011) | Children’s Hospital Bambino Gesù in Rome ethical committee |
| [1] | Agarwal Gupta, N., & Kabra, M. (2013). Diagnosis and management of Down Syndrome. The Indian Journal of Pediatrics, 81(6), 560-567. |
| [2] | Antonarakis, S. E., Skotko, B. G., Rafii, M. S., Strydom, A., Pape, S. E., Bianchi, D. W., Sherman, S. L., & Reeves, R. H. (2020). Down syndrome. Nature Reviews Disease Primers, 6(1). |
| [3] | Baliyan, V., Das, C., Sharma, R., & Gupta, A. (2016). Diffusion Weighted Imaging: Technique and Applications. World Journal of Radiology, 8(9), 785. |
| [4] | Bhargava, R., Hahn, G., Hirsch, W., Kim, M.-J., Mentzel, H.-J., Olsen, Ø. E., Stokland, E., Triulzi, F., & Vazquez, E. (2013). Contrast-enhanced magnetic resonance imaging in pediatric patients: Review and recommendations for current practice. Magnetic Resonance Insights, 6. |
| [5] | Brennan, S. E., & Munn, Z. (2021). Prisma 2020: A reporting guideline for the next generation of Systematic Reviews. JBI Evidence Synthesis, 19(5), 906-908. |
| [6] | Brown, S. S., Mak, E., & Zaman, S. (2021a). Multi-modal imaging in Down’s syndrome: Maximizing utility through innovative neuroimaging approaches. Frontiers in Neurology, 11. |
| [7] | Buysse, D. J. (2011). Clinical pharmacology of other drugs used as hypnotics. Principles and Practice of Sleep Medicine, 492-509. |
| [8] | Carducci, F., Onorati, P., Condoluci, C., Gennaro, G. D., Quarto, P. P. P., Pierallini, A., Sara, M., Miano, S., Cornia, R., & Albertini, G. (2013). Whole-brain voxel-based morphometry study of children and adolescents with Down syndrome. Functional Neurology, 28, 19-28. |
| [9] | Center, I. (2021). Down syndrome. Inspiration Center. |
| [10] | cognifit research cognifit. (2016, January 8). Brain Functions. Human Brain Functions and CogniFit. |
| [11] | Coppedè, F. (2016). Risk factors for down syndrome. Archives of Toxicology, 90(12), 2917-2929. |
| [12] | Coté, C. J., Lerman, J., Ward, R. M., Lugo, R. A., & Goudsouzian, N. (2009). Pharmacokinetics and pharmacology of drugs used in children. A Practice of Anesthesia for Infants and Children, 89-146. |
| [13] | Courchesne, E., Chisum, H. J., Townsend, J., Cowles, A., Covington, J., Egaas, B., Harwood, M., Hinds, S., & Press, G. A. (2000). Normal brain development and aging: Quantitative Analysis at in vivo MR imaging in Healthy Volunteers. Radiology, 216(3), 672-682. |
| [14] | Cuckle, H., & Maymon, R. (2016). Development of prenatal screening—a historical overview. Seminars in Perinatology, 40(1), 12-22. |
| [15] | Dhikav, V., & Anand, K. (2012). Hippocampus in health and disease: An overview. Annals of Indian Academy of Neurology, 15(4), 239. |
| [16] | DiProspero, N. D., Kim, S., & Yassa, M. A. (2022). Magnetic resonance imaging biomarkers for cognitive decline in down syndrome. The Neurobiology of Aging and Alzheimer Disease in Down Syndrome, 149-172. |
| [17] | Esbensen, A. J., Schworer, E. K., Fidler, D. J., & Thurman, A. J. (2022). Considerations for measuring individual outcomes across contexts in down syndrome: Implications for research and clinical trials. International Review of Research in Developmental Disabilities, 191-225. |
| [18] | Faber, J., & Fonseca, L. M. (2014). How sample size influences research outcomes. Dental Press Journal of Orthodontics, 19(4), 27-29. |
| [19] | Fujii, Y., Aida, N., Niwa, T., Enokizono, M., Nozawa, K., & Inoue, T. (2017). A small Pons as a characteristic finding in Down syndrome: A quantitative MRI study. Brain and Development, 39(4), 298-305. |
| [20] | Galaburda, A. M., & Schmitt, J. E. (2003). Neuroanatomical considerations specific to the study of Neurogenetics. Genetics and Genomics of Neurobehavioral Disorders, 21-38. |
| [21] | Ganzetti, M., Wenderoth, N., & Mantini, D. (2015). Mapping pathological changes in brain structure by combining T1- and T2-weighted MR imaging data. Neuroradiology, 57(9), 917-928. |
| [22] | Guihard-Costa, A.-M., Khung, S., Delbecque, K., Ménez, F., & Delezoide, A.-L. (2006). Biometry of face and brain in fetuses with trisomy 21. Pediatric Research, 59(1), 33-38. |
| [23] | Gunbey, H. P., Bilgici, M. C., Aslan, K., Has, A. C., Ogur, M. G., Alhan, A., & Incesu, L. (2016). Structural brain alterations of Down’s syndrome in early childhood evaluation by DTI and volumetric analyses. European Radiology, 27(7), 3013-3021. |
| [24] | Hamadelseed, O., & Skutella, T. (2023). Correlating MRI-Based Brain Volumetry and Cognitive Assessment in People with Down Syndrome. |
| [25] | HaVy Ngo-Hamilton, Pharm. D. (2024, September 25). Therapeutic index: What it is and why it’s important. Buzzrx. |
| [26] | Kitano, R., Madan, N., Mikami, T., Madankumar, R., Skotko, B. G., Santoro, S., Ralston, S. J., Bianchi, D. W., & Tarui, T. (2023a). Biometric magnetic resonance imaging analysis of Fetal Brain Development in down syndrome. Prenatal Diagnosis, 43(11), 1450-1458. |
| [27] |
Lee, W., & Hotopf, M. (2012). Critical appraisal Reviewing scientific evidence and reading academic papers. Core psychiatry.
https://www.sciencedirect.com/sdfe/pdf/download/eid/3-s2.0-B9781416034797100205/first-page-pdf |
| [28] | Menghini, D., Costanzo, F., & Vicari, S. (2011a). Relationship between brain and cognitive processes in down syndrome. Behavior Genetics, 41(3), 381-393. |
| [29] | Nagaoka, S. I., Hassold, T. J., & Hunt, P. A. (2012). Human aneuploidy: Mechanisms and new insights into an age-old problem. Nature Reviews Genetics, 13(7), 493-504. |
| [30] | Patkee, P. A., Baburamani, A. A., Kyriakopoulou, V., Davidson, A., Avini, E., Dimitrova, R., Allsop, J., Hughes, E., Kangas, J., McAlonan, G., & Rutherford, M. A. (2020). Early alterations in cortical and cerebellar regional brain growth in Down syndrome: An in vivo fetal and neonatal MRI assessment. NeuroImage: Clinical, 25, 102139. |
| [31] | Pinter, J. D., Eliez, S., Schmitt, J. E., Capone, G. T., & Reiss, A. L. (2001a). Neuroanatomy of down’s syndrome: A high-resolution MRI study. American Journal of Psychiatry, 158(10), 1659-1665. |
| [32] | Popay, J., Roberts, H., Sowden, A., & Duffy, S. (2006, January). guidance on the conduct of narrative synthesis in systematic reviews: A product from the ESRC methods programme. ResearchGate. |
| [33] | Rafi, I., Hill, M., Hayward, J., & Chitty, L. S. (2017). Non-invasive prenatal testing: Use of cell-free fetal DNA in Down syndrome screening. British Journal of General Practice, 67(660), 298-299. |
| [34] | Salehi, A., Wesson Ashford, J., & J. Mufson, E. (2015). Editorial (thematic issue: The link between alzheimer’s disease and Down Syndrome. A historical perspective). Current Alzheimer Research, 13(1), 2-6. |
| [35] | Shiohama, T., Levman, J., Baumer, N., & Takahashi, E. (2019). Structural magnetic resonance imaging-based brain morphology study in infants and toddlers with down syndrome: The effect of Comorbidities. Pediatric Neurology, 100, 67-73. |
| [36] | Startin, C., Startin, C. M., D’Souza, H., Ball, G., Hamburg, S., Hithersay, R., Hughes, K. M., Massand, E., Karmiloff-Smith, A., Thomas, M. S., & Strydom, A. (2020). Health comorbidities and cognitive abilities across the lifespan in down syndrome. Journal of Neurodevelopmental Disorders, 12(1). |
| [37] | Synder, D. (2022). Ethical Considerations for Clinical Trials Involving Children. |
| [38] | Tarui, T., Im, K., Madan, N., Madankumar, R., Skotko, B. G., Schwartz, A., Sharr, C., Ralston, S. J., Kitano, R., Akiyama, S., Yun, H. J., Grant, E., & Bianchi, D. W. (2019). Quantitative MRI analyses of regional brain growth in living fetuses with down syndrome. Cerebral Cortex, 30(1), 382-390. |
| [39] |
Vannais, A. L. (2009, July 1). Practice standards for the imaging of children and young. doc Library.
https://www.sor.org/download-file?f=21ee42cf-d62d-46c2-a125-f570f6990494&t=m |
| [40] | Yun, H. J., Perez, J. D., Sosa, P., Valdés, J. A., Madan, N., Kitano, R., Akiyama, S., Skotko, B. G., Feldman, H. A., Bianchi, D. W., Grant, P. E., Tarui, T., & Im, K. (2020). Regional alterations in cortical sulcal depth in living fetuses with down syndrome. Cerebral Cortex, 31(2), 757-767. |
| [41] | Śmigielska-Kuzia, J., Boćkowski, L., Sobaniec, W., Sendrowski, K., Olchowik, B., Cholewa, M., łukasiewicz, A., & łebkowska, U. (2011). A volumetric magnetic resonance imaging study of brain structures in children with down syndrome. Neurologia i Neurochirurgia Polska, 45(4), 363-369. |
APA Style
Halaweh, R. N. (2025). Magnetic Resonance Imaging in the Detection of Neuroanatomical Changes in Down Syndrome: A Narrative Review from the Developing Fetus to Childhood. American Journal of Pediatrics, 11(2), 81-92. https://doi.org/10.11648/j.ajp.20251102.18
ACS Style
Halaweh, R. N. Magnetic Resonance Imaging in the Detection of Neuroanatomical Changes in Down Syndrome: A Narrative Review from the Developing Fetus to Childhood. Am. J. Pediatr. 2025, 11(2), 81-92. doi: 10.11648/j.ajp.20251102.18
AMA Style
Halaweh RN. Magnetic Resonance Imaging in the Detection of Neuroanatomical Changes in Down Syndrome: A Narrative Review from the Developing Fetus to Childhood. Am J Pediatr. 2025;11(2):81-92. doi: 10.11648/j.ajp.20251102.18
@article{10.11648/j.ajp.20251102.18,
author = {Raneem Nabil Halaweh},
title = {Magnetic Resonance Imaging in the Detection of Neuroanatomical Changes in Down Syndrome: A Narrative Review from the Developing Fetus to Childhood
},
journal = {American Journal of Pediatrics},
volume = {11},
number = {2},
pages = {81-92},
doi = {10.11648/j.ajp.20251102.18},
url = {https://doi.org/10.11648/j.ajp.20251102.18},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20251102.18},
abstract = {Background: Down syndrome (DS) or trisomy 21 is a genetic disorder caused by unusual cell division and an extra copy of chromosome 21. DS is characterized by phenotypic characteristics identified clinically and is the most common genetic cause of intellectual disability in children. DS can also result in other medical complications that involve the heart, the digestive system and memory disabilities leading to Alzheimer’s disease (AD). Although diagnosis is made clinically, screening tests such as chorionic villus sampling (CVS), amniocentesis and ultrasound detecting translucency of the nuchal folds of the neck are used to detect it at its early stages. There is no known treatment for DS, however, early detection and intervention can improve quality of life (QoL) for patients and their parents. Aims: This review aims to identify the importance of neuroimaging, particularly magnetic resonance imaging (MRI), in early diagnosis of DS. The review will explore how neuroanatomical changes can guide future research and focus interventions to target needs of individuals. Method: This review included 12 studies on DS from the year 2000 to date. Participants included ranged from fetus to 15-year-old teenagers. Diagnosis of DS was first made by CVS, amniocentesis or ultrasound depending on mother’s preference followed by karyotyping confirming trisomy 21. The main imaging modality included in the review is high-resolution MRI which all participants underwent for comparison. Results: Results of the MRI showed an overall reduction in volume in different areas of the brain in DS patients compared to controls. Most prominent volume reduction were found in the frontal lobes, hippocampus and brainstem. With increasing age there was preservation of volumes in parietal and temporal lobes. After the age of 11 years, changes in the grey and white matters started to appear. Conclusion: Early detection of brain changes, especially in fetus, could improve developmental outcomes for people suffering from DS by providing early and tailored interventions focusing on potential cognitive impairments associated to damaged brain areas. These neuroanatomical changes in DS patients are correlated to cognitive disabilities that are controlled by specific areas of the brain, relating this review to its clinical relevance. Some limitations of the studies included in the review was the small sample size. Selection bias was introduced by recruiting participants solely from hospitals where healthcare access might be limited to those can afford it. Some strengths include the consistency in diagnosing DS first with chorionic villus sampling, amniocentesis and ultrasound and confirmation it with karyotyping.
},
year = {2025}
}
TY - JOUR T1 - Magnetic Resonance Imaging in the Detection of Neuroanatomical Changes in Down Syndrome: A Narrative Review from the Developing Fetus to Childhood AU - Raneem Nabil Halaweh Y1 - 2025/05/19 PY - 2025 N1 - https://doi.org/10.11648/j.ajp.20251102.18 DO - 10.11648/j.ajp.20251102.18 T2 - American Journal of Pediatrics JF - American Journal of Pediatrics JO - American Journal of Pediatrics SP - 81 EP - 92 PB - Science Publishing Group SN - 2472-0909 UR - https://doi.org/10.11648/j.ajp.20251102.18 AB - Background: Down syndrome (DS) or trisomy 21 is a genetic disorder caused by unusual cell division and an extra copy of chromosome 21. DS is characterized by phenotypic characteristics identified clinically and is the most common genetic cause of intellectual disability in children. DS can also result in other medical complications that involve the heart, the digestive system and memory disabilities leading to Alzheimer’s disease (AD). Although diagnosis is made clinically, screening tests such as chorionic villus sampling (CVS), amniocentesis and ultrasound detecting translucency of the nuchal folds of the neck are used to detect it at its early stages. There is no known treatment for DS, however, early detection and intervention can improve quality of life (QoL) for patients and their parents. Aims: This review aims to identify the importance of neuroimaging, particularly magnetic resonance imaging (MRI), in early diagnosis of DS. The review will explore how neuroanatomical changes can guide future research and focus interventions to target needs of individuals. Method: This review included 12 studies on DS from the year 2000 to date. Participants included ranged from fetus to 15-year-old teenagers. Diagnosis of DS was first made by CVS, amniocentesis or ultrasound depending on mother’s preference followed by karyotyping confirming trisomy 21. The main imaging modality included in the review is high-resolution MRI which all participants underwent for comparison. Results: Results of the MRI showed an overall reduction in volume in different areas of the brain in DS patients compared to controls. Most prominent volume reduction were found in the frontal lobes, hippocampus and brainstem. With increasing age there was preservation of volumes in parietal and temporal lobes. After the age of 11 years, changes in the grey and white matters started to appear. Conclusion: Early detection of brain changes, especially in fetus, could improve developmental outcomes for people suffering from DS by providing early and tailored interventions focusing on potential cognitive impairments associated to damaged brain areas. These neuroanatomical changes in DS patients are correlated to cognitive disabilities that are controlled by specific areas of the brain, relating this review to its clinical relevance. Some limitations of the studies included in the review was the small sample size. Selection bias was introduced by recruiting participants solely from hospitals where healthcare access might be limited to those can afford it. Some strengths include the consistency in diagnosing DS first with chorionic villus sampling, amniocentesis and ultrasound and confirmation it with karyotyping. VL - 11 IS - 2 ER -
Institute of Psychiatry, Psychology and Neuroscience, King’s College London, United Kingdom, London
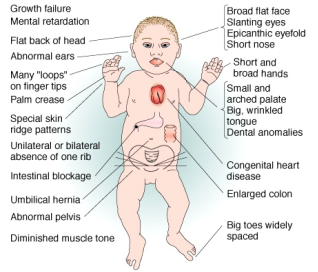
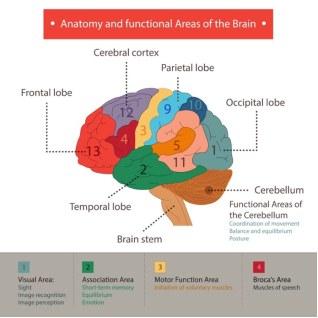
Figure 2. Areas of the brain and their related cognitive function [10].
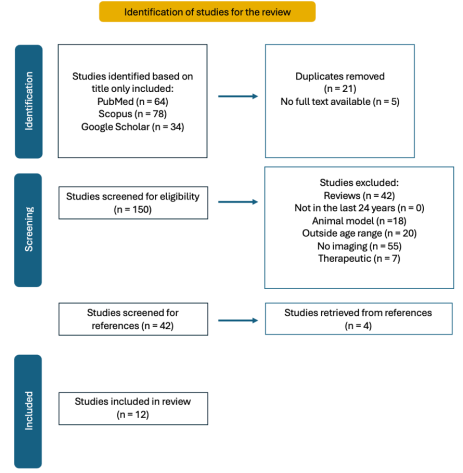
Figure 3. PRISMA flowchart showing screening method adapated for the review [5].
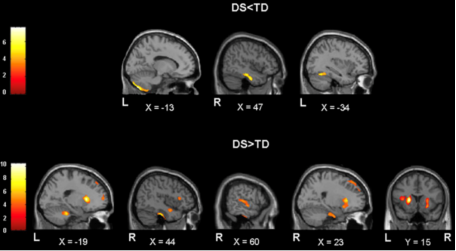
Figure 4. Difference in volume densities in 11 to 15 years of age patients with DS compared to controls in different parts of the brain. The top part of the figure shows controls with more grey matter volume illustrated by increased densities in some areas of the brain compared to increased grey matter densities detected in DS patients in other brain regions shown at the bottom. Overall, there is a reduction in volumes of left posterior cerebellum, right inferior temporal gyrus, right and left medial temporal lobes in DS patients [28].

