1. Introduction
Stroke is defined as a sudden loss of brain function caused by a decreased cerebral blood flow. Stroke is an acute onset neurological sign or symptom attributable to focal brain infarction or hemorrhage, as rapidly developing clinical signs of focal or global disturbance of cerebral function. A stroke is an acute neurological emergency with the need of urgent diagnosis, central nervous system Imaging and prompt treatment, ideally in the set time window. Stroke can occur at all life stages but pathophysiology, clinical presentation and prognostic are variable depending on the patient’s age. A stroke in pediatric patients is associated with significant morbidity and mortality
| [1] | Rosa M., De Lucia S., Rinaldi V. E., Le Gal J., Desmarest M., Veropalumbo C., et al. Paediatric arterial ischemic stroke: acute management, recent advances and remaining issues. Ital J Pediatr. 2015; 41: 1–12. |
| [2] | Klučka J., Klabusayová E., Musilová T., Kramplová T., Skříšovská T., Kratochvíl M., et al. Pediatric patient with ischemic stroke: initial approach and early management. Children. 2021; 8(8): 649. |
[1, 2]
The occurrence of ischemic stroke in pediatric populations, despite it rarity, implicates age-dependent peculiarities in term of risk factors, etiopathogenesis, clinical presentations, and therapeutic approaches.
| [3] | Mastrangelo M., Giordo L., Ricciardi G., De Michele M., Toni D., Leuzzi V. Acute ischemic stroke in childhood: a comprehensive review. Eur J Pediatr. 2022; 1–14. |
[3]
Childhood stroke is often underdiagnosed, estimates of incidence of childhood stroke occurs in approximately 1,3-13 per 100,000 children per year, the highest published incidence is below five years with a median age of 2,3 years.
| [2] | Klučka J., Klabusayová E., Musilová T., Kramplová T., Skříšovská T., Kratochvíl M., et al. Pediatric patient with ischemic stroke: initial approach and early management. Children. 2021; 8(8): 649. |
[2]
Approximately 20% of children die after an ischemic stroke while more than 50% of those surviving present neurological sequelae most commonly hemiparesis. The cumulative stroke recurrence rate has been reported to be 15% at 1 year, 19% at 5 years, and up to 40% at 5 years
| [4] | Ciccone S., Cappella M., Borgna-Pignatti C. Ischemic stroke in infants and children: practical management in emergency. Stroke Res Treat. 2011; 2011(1): 736965. |
[4].
There are two major subtypes of stroke are ischemic and hemorrhagic. While adult strokes are prevalently ischemic (80%) and due to atherosclerosis, in childhood up to 45% of stroke are hemorrhagic and are associated with wide spectrum of risk factors.
| [4] | Ciccone S., Cappella M., Borgna-Pignatti C. Ischemic stroke in infants and children: practical management in emergency. Stroke Res Treat. 2011; 2011(1): 736965. |
[4]
Ischemic stroke includes arterial ischemic stroke and venous infarction caused by cerebral sinovenous thrombosis (CSVT) or cortical vein thrombosis. The age related classification of ischemic stroke divides this clinical syndrome into two categories: perinatal stroke (sometimes referred to as neonatal stroke) and childhood stroke. Perinatal or neonatal stroke as stroke occurs during the perinatal period from 20 weeks-28 weeks of gestation until the end of the newborn period (28th postnatal day). Childhood stroke encompasses the age group from 28 days up to 18 years of age
| [2] | Klučka J., Klabusayová E., Musilová T., Kramplová T., Skříšovská T., Kratochvíl M., et al. Pediatric patient with ischemic stroke: initial approach and early management. Children. 2021; 8(8): 649. |
[2].
The diagnosis of stroke in children can be difficult and is often delayed because sign and symptoms can be subtle and nonspecific, there are many other diseases that may mimic a stroke in children. History and clinical examination should exclude underlying diseases or predisposing factors. Neuroimaging is crucial in defining diagnosis. Others test might be necessary, according to the clinical picture
| [4] | Ciccone S., Cappella M., Borgna-Pignatti C. Ischemic stroke in infants and children: practical management in emergency. Stroke Res Treat. 2011; 2011(1): 736965. |
[4]
The age-related variable clinical presentation could result in a delay in diagnosis and could negatively influence the overall outcome. The early management should be based on early recognition, early neurologic examination together with neuroimaging (preferable magnetic resonance imaging-MRI). The treatment is based on supportive therapy in combination with intravenous/intraarterial thrombolytic therapy and/or mechanical thrombectomy in selected cases
| [2] | Klučka J., Klabusayová E., Musilová T., Kramplová T., Skříšovská T., Kratochvíl M., et al. Pediatric patient with ischemic stroke: initial approach and early management. Children. 2021; 8(8): 649. |
[2].
2. Case Report
A 2 years-old girl child was admitted to the outpatient clinic at Ngoerah Hospital with a chief complain of weakness on the left hand and leg which persisted since 1 year prior to hospital admission. The parents realized that the complain began when the patient started to crawl at the age of 9 months. Since then, the patient’s left hands have always been grasping and difficult to move. A few months later when she started learning to walk, she found that her left leg was weak, and the patient walked on her tiptoes and clawed finger foot. The patient was still able to do her daily activities using her right hand. There was no prior complain of seizure, fever, vomit, nausea. There was no history of artheriopaties, chronic systemic disease with inflammation, sickle cell anemia, cardiac diseases and hypercoagulable states (thrombophilia), metabolic diseases, trauma, infection, dehydration, and cancer. She had no pertinent past medical history. Patient’s mother had a history of seizures in childhood and was taking anti- epileptic medication for 2 years. Family history of cardiovascular disease was denied.
She was born to non-consanguineous parents and had an uneventful antenatal and perinatal history. She was born by cesarean section, term baby, immediately cried with birth weight of 3200 grams. Growth and development history were convenient with milestone.
Physical examination when the patient first came to the outpatient clinic revealed that patient was conscious, the body temperature 36,50C, heart rate 92 beats per minute, respiratory rates was regular 22 times per minute, and the oxygen saturation were normal (99% room air). Her nutritional status was well nourished according to her anthropometry. The patient had normal head circumference. General physical examination showed normal cardiovascular and respiratory system and normal abdominal examination. Neurologic examination showed symmetrical right and left facial muscle, normal vision and hearing, and other cranial nerves were normal. Neurology status: GCS E4V5M6, round and isochoric pupil 3/3 mm, light refleks (+/+), meningeal sign (-). Motoric examination revealed decreased grip strength of the left hand, and strength of left leg decreased. Pathological reflex, babinski negative/negative, chaddok negative/negative, Oppenheim negative/negative.
Laboratory examination at RSUP Prof. Dr. I.G.N.G Ngoerah Hospital September 06th 2022, leukocyte count was 8.55 K/μL (neutropil 30.10%, lymphocyte 61.30%), hemoglobin level was 11.30 g/dL (MCV 77.50 fl; MCH 25.40 pg; MCHC 32.80 g/dl); hematocrit was 34.50%; platelet count was 365 K/μL, with impression normal limit. and electrolyte, sodium was 138 mmol/L, potassium was 3,64 mmol/, chloride was 106,6 mmol/, calcium was 8,6 with impression normal limit. renal function BUN: 11,6 mg/gl, creatinine 0,6 mg/dl, GFR 156,7 with impression normal limit. Laboratory examination at RSUP Prof. Dr. I.G.N.G Ngoerah Hospital May 14th 2024, cholesterol total was 134 mg/dL, cholesterol LDL was 88 mg/dL, cholesterol HDL was 46 mg/dL, triglyceride was 89 mg/dL with impression normal limit. The results of Vitamin D examination are 27.8 ng/mL with impression vitamin D insufficiency. Echocardiography revealed normal result.
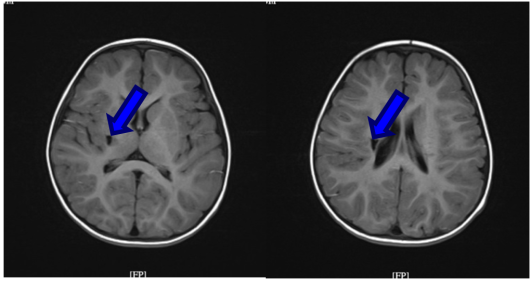
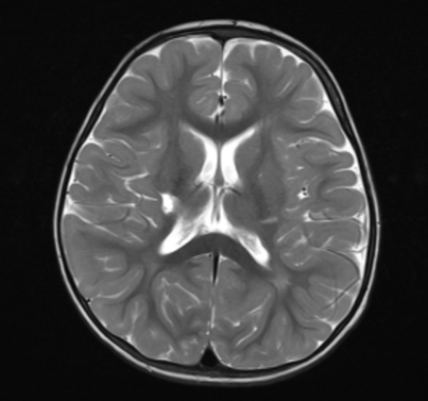
Magnetic resonance imaging (MRI) revealed there are well defined lesions on the corona radiata and right lentiform nucleus, appear hypointense on T1/FLAIR, hyperintense on T2, on DWI/ADC, no restricted diffusion is seen, on SWI phase images no blooming artefacts are seen. Sulci and gyri, ventricular system and cysterna were normal. T2WI hyperintensity was seen in the ethmoidal, right and left maxillary sinuses, right inferior nasal concha hypertrophy was seen, nasal septum deviation was not seen, concha nasi was not hypertrophied, and SCALP no abnormality was seen.
Figure 1. MRI T1 Sequence.
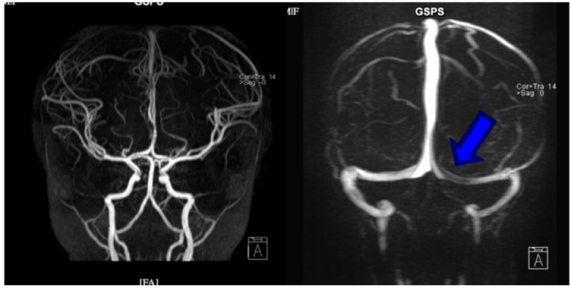
Magnetic resonance arteriography (MRA) showed: left-right ICA and MCA look of normal caliber and shape, no stenosis, aneurysm or AVM. AComA is not visualized, as a normal variant. PCOm, ACA, PCA, basal artery and right and left vertebral arteries looked of normal caliber and shape, no stenosis, aneurysm or AVM were seen. Head Magnetic resonance venography (MRV) revealed: there was a lack of flow in part of the left transverse sinus. Sinus sagitalis superior inferior, right and left transverse sinus, right and left internal jugular vein, right and left cavernous sinus, sigmoid sinus right and left, internal cerebral vein, vein of Gallen straight and torcula herophilia looks good. Conclusion of Magnetic resonance imaging examination showed chronic ischemic cerebral infarction in corona radiata, right lentiform nucleus, right and left ethmoidal and maxillary sinusitis. Observation lack of flow in the left transverse sinus, suspected left transverse sinus thrombosis. It is recommended to do a cerebral digital subtraction angiography (DSA) examination.
The patient was diagnosed with ischemic stroke, left hemiparesis et cause chronic ischemic cerebral infarction in radiata corona based on her clinical and radiological findings. The patient was advised to undergo DSA examination, but the parents refused to do DSA for unknown reason.
Figure 2. MRA Brain Arteries and Vena.
Patient continued the follow up at outpatient clinic and had physiotherapy session regularly. One year after the follow up period, patient had complain of seizure. The patient experienced a seizure characterized by whole-body stiffness, with jerking movement, lasting approximately 5 minutes. Electroencephalography was performed showing mild generalized hypofunction with generalized epileptic waves (Abnormal III).
The patient was diagnosed with epilepsy motor tonic clonic with structural etiology, comorbid ischemic stroke. The patient was given valproic acid with a dosage of 20 mg/kg/day every 12 hours. Seizure were controlled by administering valproic acid medication. The patient was continued to be followed up at the neurology outpatient clinic.
Figure 4. Electroencephalography Results.
3. Discussion
In this Stroke in children is a relatively rare event, but it is a leading cause of acquired brain injury in this population. The incidence of pediatric stroke is approximately 1.2 to 13 cases per 100,000 children under 18, but due to potential misdiagnoses or a lack of clinical suspicion and workup, these estimates are likely low.
| [5] | Tsze D. S., Valente J. H. Pediatric stroke: a review. Emerg Med Int. 2011; 2011(1): 734506. |
[5]
Ischemic strokes are more common in children, often resulting from either embolic or thrombotic events, while hemorrhagic strokes can also occur, particularly in the context of vascular malformations, trauma, or bleeding disorders. A higher predisposition to an earlier onset was highlighted in Asian and black children, because of a higher incidence of concurrent chronic disorders (with a relative risk of 2.14 and 2.28, respectively, for Asian and black children, compared to 1.34 of other ethnicities).
| [6] | Mallick A. A., Ganesan V., Kirkham F. J., Fallon P., Hedderly T., McShane T., et al. Childhood arterial ischaemic stroke incidence, presenting features, and risk factors: a prospective population-based study. Lancet Neurol. 2014; 13(1): 35–43. |
[6]
To know the risk factors of stroke in pediatric population, we perform journal searching and found the journal titled “
Epidemiology, Risk Factors, and Characteristics of Pediatric Stroke: A Nationwide Population-Based Study”. This study revealed that infants age <2 years have a significantly higher prevalence and incidence of stroke (p<0.001, p<0.001). In socioeconomic status analysis, children in lowest household income level has higher prevalence (p<0.05).
| [7] | Chiang K. L., Cheng C. Y. Epidemiology, risk factors and characteristics of pediatric stroke: A nationwide population-based study. QJM An Int J Med. 2018; 111(7): 445–54. |
[7]
In this case, patient was a 2 years old Asian girl admitted to the outpatient clinic with left hemiparesis since 1 year prior to hospital admission. The patient’s age (<2 years old) and Asian decent may be the risk factors of this patient to develop ischemic stroke.
There are various cause of acute ischemic stroke (AIS) in children. The Childhood AIS Standardized Classification and Diagnostic Evaluation (CASCADE) criteria are used to categorize strokes according to the underlying causes and arteriopathies are recognized as the most significant risk for childhood AIS (
Figure 1).
| [8] | Bernard T. J., Manco-Johnson M. J., Lo W., MacKay M. T., Ganesan V., Deveber G., et al. Towards a consensus-based classification of childhood arterial ischemic stroke. Stroke. 2012; 43(2): 371–7. |
[8]
Blood vessel abnormalities may be either chronic or temporary/acute changes, and they are frequently detected through vascular imaging. Etiologic factors of AIS, whether congenital or acquired—such as heart disease, metabolic imbalances, thrombophilia, and autoimmune conditions like systemic lupus erythematosus—may or may not cause noticeable changes on imaging. Arteriopathy is defined as the imaging appearance of an in-situ arterial abnormality (ie, stenosis, irregularity, occlusion, banding, pseudoaneurysm, dissection flap) that is not attributable to an exogenous thrombus (e.g., cardioembolism) and is not considered a normal developmental variant. The term focal cerebral arteriopathy (FCA) is broadly used to describe transient cerebral arteriopathy (TCA) and other vascular conditions classified under the CASCADE criteria for AIS. TCA is characterized by localized narrowing or stenosis of the vessel walls, typically occurring in the distal internal carotid artery, proximal middle cerebral artery, or the circle of Willis. These imaging findings are more frequently observed in children with abnormal lipid levels or a family history of cardiovascular disease. Studies suggest a connection between TCA and infections such as varicella, acute herpes viruses, and other upper respiratory infections; however, the role of inflammatory pathways in TCAs is not yet fully understood.
| [8] | Bernard T. J., Manco-Johnson M. J., Lo W., MacKay M. T., Ganesan V., Deveber G., et al. Towards a consensus-based classification of childhood arterial ischemic stroke. Stroke. 2012; 43(2): 371–7. |
[8]
In this case, the exact cause of acute ischemic stroke cannot be confirmed as the patient came to the hospital more than 1 year after the stroke episode. Patient’s physical examination showed normal cardiac function and echocardiography confirmed the normal heart structure and function, ruling out cardiac abnormalities as the cause of acute ischemic stroke in the patient. Patient had normal platelet count, ruling out thrombophilia as the cause of acute ischemic stroke. Patient also had normal lipid profiles and there were no history of familial cardiovascular disease. Patient’s parents also denied any history of infections prior to the stroke episode, thus, infection may not be the cause of ischemic stroke in this patient. Arteriopathies, the most common cause of stroke in children, is likely to be the cause of stroke in the patient.
| [8] | Bernard T. J., Manco-Johnson M. J., Lo W., MacKay M. T., Ganesan V., Deveber G., et al. Towards a consensus-based classification of childhood arterial ischemic stroke. Stroke. 2012; 43(2): 371–7. |
[8]
Childhood stroke may present with several localizing signs and symptom such as hemiparesis or hemifacial weakness, speech or language dysfunctions, vision disturbances, or ataxia, and non-localizing manifestations. Non-localizing manifestations and seizures have a higher frequency in pediatric age, especially in children under the age of 6.
| [6] | Mallick A. A., Ganesan V., Kirkham F. J., Fallon P., Hedderly T., McShane T., et al. Childhood arterial ischaemic stroke incidence, presenting features, and risk factors: a prospective population-based study. Lancet Neurol. 2014; 13(1): 35–43. |
| [9] | Ferriero D. M., Fullerton H. J., Bernard T. J., Billinghurst L., Daniels S. R., DeBaun M. R., et al. Management of stroke in neonates and children: a scientific statement from the American Heart Association/American Stroke Association. Stroke. 2019; 50(3): e51–96. |
[6, 9]
Diffuse signs have a more variable distribution in the different age ranges: seizures appear in more than half of infants under the age of 12 months (56–75%), whereas headache is a frequent complaint in school-age children (33–50%). In this case, the patient presented with left hemiparesis and denied any history of speech or visual disturbance, headache, altered mental status, and seizure.
Initial management of stroke in children should focus on early detection and correctly diagnosing the type of stroke, along with immediate stabilization and resuscitation. Correction of underlying conditions such as hypoxia, febrility, hypoglycemia, or significant metabolic derangements are imperative. As mentioned, most children have no previous known risk factors for acute ischemic stroke. Computed tomography (CT) imaging is frequently unrevealing early in ischemic stroke and if suspicion remains high.
| [2] | Klučka J., Klabusayová E., Musilová T., Kramplová T., Skříšovská T., Kratochvíl M., et al. Pediatric patient with ischemic stroke: initial approach and early management. Children. 2021; 8(8): 649. |
[2]
The initial CT scan in children could be falsely negative, may missed AIS diagnosis in 44-83% of patient cases, and can miss hyperacute small lesions or lesions located in the posterior fossa and brainstem.
| [3] | Mastrangelo M., Giordo L., Ricciardi G., De Michele M., Toni D., Leuzzi V. Acute ischemic stroke in childhood: a comprehensive review. Eur J Pediatr. 2022; 1–14. |
[3]
Magnetic resonance imaging (MRI) has exquisite sensitivity for identification of infarction.
| [10] | Hollist M., Au K., Morgan L., Shetty P. A., Rane R., Hollist A., et al. Pediatric stroke: overview and recent updates. Aging Dis. 2021; 12(4): 1043. |
[10]
Magnetic Resonance Imaging remains the gold standard for the investigation of arterial ischemic stroke in infants and children, due to its greater sensitivity and specificity.
| [1] | Rosa M., De Lucia S., Rinaldi V. E., Le Gal J., Desmarest M., Veropalumbo C., et al. Paediatric arterial ischemic stroke: acute management, recent advances and remaining issues. Ital J Pediatr. 2015; 41: 1–12. |
[1]
Magnetic resonance (MR) is useful to differentiate stroke from stroke mimics.
| [4] | Ciccone S., Cappella M., Borgna-Pignatti C. Ischemic stroke in infants and children: practical management in emergency. Stroke Res Treat. 2011; 2011(1): 736965. |
[4]
Early treatment of suspected ischemic infarct should not be delayed in order to obtain MRI imaging, but it is rarely available in the hyperacute phase managed in emergency departments.
| [10] | Hollist M., Au K., Morgan L., Shetty P. A., Rane R., Hollist A., et al. Pediatric stroke: overview and recent updates. Aging Dis. 2021; 12(4): 1043. |
[10]
Computed tomography (CT) imaging remains the modality of choice for acute presentation of focal neurologic deficits. It has very high sensitivity for identifying acute hemorrhage and can also assist the clinician in rapidly narrowing the differential diagnosis. Computed tomography (CT) is usually normal within the first 12 hours after the onset of symptoms.
| [5] | Tsze D. S., Valente J. H. Pediatric stroke: a review. Emerg Med Int. 2011; 2011(1): 734506. |
[5]
Magnetic resonance with diffusion weighting is very useful in accurately identifying regions of early ischemic and infarction. Typical MRI findings in patients with acute cerebral ischemia include hypertense signal in white matter on T2-weighted image and fluid-attenuated in version recovery images, with a resultant loss of grey matter-white matter differentiation. Other finding may be sulcal effacement and mass effect, loss of the arterial flow voids and stasis of contrast material within vessels in the affected territories.
| [1] | Rosa M., De Lucia S., Rinaldi V. E., Le Gal J., Desmarest M., Veropalumbo C., et al. Paediatric arterial ischemic stroke: acute management, recent advances and remaining issues. Ital J Pediatr. 2015; 41: 1–12. |
[1]
Magnetic resonance angiography (MRA) and CT angiography (CTA) are increasingly being used to detect arterial abnormalities. Currently, MRA is the first line screening imaging used in most institution. MRA has the advantage of indirectly visualizing the vessel wall and the lumen and sparing the patient radiation.
| [9] | Ferriero D. M., Fullerton H. J., Bernard T. J., Billinghurst L., Daniels S. R., DeBaun M. R., et al. Management of stroke in neonates and children: a scientific statement from the American Heart Association/American Stroke Association. Stroke. 2019; 50(3): e51–96. |
[9]
In this case, patient already had MRI with contrast last year which revealed there are well-defined lesion on the corona radiata and right lentiform nucleus, appear hypointense on T1/FLAIR, hyperintense on T2, on DWI/ADC no restricted diffusion is seen, on SWI phase images no blooming artefacts are seen. Head MRA and MRV showed chronic ischemic cerebral infarction in corona radiata and right lentiform nucleus, as well as, lack of flow in the left transverse sinus suggesting left transverse sinus thrombosis.
Besides conventional angiography, recent studies showed that DSA had been recommended for diagnosis of ischemic stroke. DSA could provide more detailed visualization of the craniofacial and intracranial vasculature, thus becoming the modality of choice for imaging cranial vasculature. However, utilization of DSA in pediatric stroke patients was still limited due to concerns regarding its invasive nature and higher radiation exposure.
| [11] | Chulpayev B., Benitez S., Van Dine S., Erdfarb A. J., Moshé S. L., Ballaban-Gil K., et al. Pediatric Ischemic Strokes. Adv Clin Radiol. 2020; 2: 319–24. |
[11]
A previous study involving 241 consecutive pediatric cases who underwent cerebral DSA showed that this procedure was very safe, with no intraprocedural complications and very low post-procedural complications (0.4%). In this case, the patient was advised to undergo DSA because the results of other examinations were inconclusive and could not determine the exact cause of AIS in the patient. However, the parents refused, so DSA was not performed on this patient.
In acute ischemic stroke, irreversible brain tissue ischemia occurs within minutes to hours of arterial occlusion. Therefore, rapid management is required in order to increase brain tissue survival primarily in the penumbra. Arterial recanalization therapy, including intravenous tissue-type plasminogen activator (tPA) and intra-arterial tPA or endovascular thrombectomy, has been shown to significantly benefit adults with AIS when implemented within discrete time windows. Until now, randomized clinical trial assessing safety and efficacy of thrombolysis and/or endovascular treatment were never performed for pediatric age.
However, according to the pediatric stroke guidelines, it is feasible to apply Recombinant Tissue Plasminogen Activator (rTPA) for the treatment of ischemic stroke in children from 2 years of age, with persistent disabling neurological deficits (e.g., Pediatric NIH Stroke Scale score ≥ 6 at the time of intervention) and radiographically confirmed cerebral large artery occlusion, within 4.5 h of known onset of symptoms.
| [9] | Ferriero D. M., Fullerton H. J., Bernard T. J., Billinghurst L., Daniels S. R., DeBaun M. R., et al. Management of stroke in neonates and children: a scientific statement from the American Heart Association/American Stroke Association. Stroke. 2019; 50(3): e51–96. |
[9]
The suggested drug dosage is the same used for adults, although according to known age-related differences in the fibrinolytic system with children having higher levels of tissue plasminogen inhibitor than adults, it would be reasonable to consider that children might benefit of higher dosages of rTPA.
The long-term treatment is commonly based on low-molecular weight heparins or acetylsalicylic acid without clear data suggesting which one of the two therapies is better in children and safety data supporting both approaches. A longer-term prevention therapy should be considered in patients with genetically determined thrombophilia (e.g., hyperhomocysteinemia, protein C deficiency, antithrombin deficiency) or in children with a stroke following congenital heart diseases, while in the other cases, the duration of the treatment may depend on the underlying aetiology with a usual preferred temporal range between 2 years and a lifetime. No data about the prophylactic use of direct oral anticoagulants (e.g., antithrombin agent or anti–factor Xa agents) in the paediatric age were collected. Specific prevention therapies may be considered for selected aetiologies (e.g., transfusions or hydroxyurea for sickle cell disease, L-arginine for MELAS, agalsidase or migalastat for Fabry disease, pyridoxine in combination with folic acid and vitamin B12, methionine-restricted, cystine-supplemented diet and betaine, for homocystinuria) even if adequate supporting evidences are often not available because of their rare occurrence. The usefulness of other specific strategies (e.g., anticoagulation for pediatric arterial dissection, patent foramen ovale closure, steroids for focal cerebral arteriopathies, or surgical strategies for moyamoya) remain unsolved controversial.
| [9] | Ferriero D. M., Fullerton H. J., Bernard T. J., Billinghurst L., Daniels S. R., DeBaun M. R., et al. Management of stroke in neonates and children: a scientific statement from the American Heart Association/American Stroke Association. Stroke. 2019; 50(3): e51–96. |
[9]
In this case, patient already presented with chronic ischemic stroke and the etiology remains uncertain, thus, we still do not consider giving long term prevention therapy for this patient.
Pediatric arterial ischemic stroke, a significant source of pediatric neurologic morbidity, can lead to numerous debilitating consequences such as sensorimotor deficits, behavioral problems, intellectual disability, language impairment, and epilepsy. Epilepsy is one of the most prominent consequences of arterial ischemic stroke in children. Previous studies show that the frequency of PSE in children is between 7 % to 41 %.
| [12] | Yücel G., Arslan A. K., Özgör B., Güngör S. Risk factors for epilepsy following arterial ischemic stroke childhood: A retrospective cohort study. Epilepsy Behav. 2024; 157: 109873. |
[12]
To know the risk factors of epilepsy after ischemic stroke in children, we perform journal searching and found the journal by Yucel, et al. entitled “Risk factors for epilepsy following arterial ischemic stroke childhood: A retrospective cohort study.” This study found that the risk factors associated with the development of post-stroke epilepsy are very early seizures (within the first six hours), high stroke severity, cortical lesions, neurological deficits, and low serum vitamin D levels were detected (p = 0.05, p = 0.036, p = 0.011, p < 0.001, p < 0.001, respectively). The association between low vitamin D and post-stroke epilepsy is through calcium homeostasis. Vitamin D can reduce neuron death through L-type voltage-dependent calcium channels in the brain and has neuroprotective and immunomodulatory effects. Thus, low vitamin D levels could increase the risk of post-stroke epilepsy. Acute seizures that develop during and/or in the first hours of a stroke may contribute to the development of post-stroke epilepsy by worsening neurodegeneration due to stroke and ischemia. Cortical involvement and more severe stroke could increase extracellular glutamate levels from the damaged neuron and an increased risk of secondary neuron damage due to excitotoxicity, resulting in hyperexcitability neuron and seizure. The presence of focal neurological deficit is also associated with post-stroke epilepsy because neurological deficit indicates more severe brain damage.
| [12] | Yücel G., Arslan A. K., Özgör B., Güngör S. Risk factors for epilepsy following arterial ischemic stroke childhood: A retrospective cohort study. Epilepsy Behav. 2024; 157: 109873. |
[12]
In this case: the patient had focal neurological deficits and vitamin D insufficiency. Therefore, this patient had higher risk of post-stroke epilepsy. Close monitoring and neuroprotective strategies might be needed in this patient.
Several factors may influence the recovery and outcomes in pediatric stroke patients, as evidenced by the study by Felling et al. entitled "Predicting Recovery and Outcome after Pediatric Stroke: Results from the International Pediatric Stroke Study." This multicenter prospective cohort study involved 587 pediatric stroke patients in 58 centers from 24 countries. At 2 years of follow-up, 46% of patients recovered, 39% showed no change, and 15% showed an emerging deficit. Stroke was recurrence in 8.2% of cases, where all recurrence cases were childhood stroke patients. Moderate-severe neurological deficit at discharge and 2 years were higher in children than neonates (9.8% vs. 48.8% and 8.0% vs. 24.7%, respectively). Further analysis found that significant predictors of poor outcome in pediatric stroke were age between 28 days and 1 year (aOR= 3.58; 95%CI =1.18-10.8; p = 0.024), underlying chronic disorder (aOR=2.23; 95%CI =1.17-4.27; p=0.015), and involvement of both small and large vascular territories (aOR = 2.84; 95%CI = 1.14-7.11; p=0.025). The significant influence of age at the time of stroke on outcomes and recovery of pediatric stroke patients proved that there was a limited period of enhanced neuroplasticity. Better brain neuroplasticity was found in children aged less than 1 year. Thus, they have better outcomes regardless of the severity of the stroke.
| [13] | Felling R. J., Rafay M. F., Bernard T. J., Carpenter J. L., Dlamini N., Hassanein S. M. A., et al. Predicting Recovery and Outcome after Pediatric Stroke: Results from the International Pediatric Stroke Study. Ann Neurol. 2020; 87(6): 840–52. |
[13]
In this case, patient had a poor outcome characterized by persistent limb weakness at 1 year after onset. Even though she did not have any underlying disease and the stroke only involved small vessels in corona radiata, persistent neurological deficits may occur because she had a stroke before one year old, and no treatment was given until she was 2 years old. It was suggested that brain plasticity in children had a U-shaped curve, with the most vulnerable period occurring between 28 days and 1 year of age. This patient had a stroke at the most susceptible period (before one year of age), while there was no specific treatment to enhance neuroplasticity after that. Thus, this may explain why the patient in this case had a poor prognosis and persistent neurological deficit. Noninvasive stimulation-based rehabilitative techniques were essential in this case and should be initiated as early as possible to modify neuroplasticity and alleviate the weakness in her limbs.
Recent studies reported a mortality rate after childhood stroke between 2.6 and 5%. Risk of mortality is even higher in patient with recurrent stroke. Not only affecting mortality risk, the recurrence of stroke will also cause a significant decrease in the quality of life in the survivors. However, studies showed that up to 25% of children will have recurrent strokes following the first event.
| [10] | Hollist M., Au K., Morgan L., Shetty P. A., Rane R., Hollist A., et al. Pediatric stroke: overview and recent updates. Aging Dis. 2021; 12(4): 1043. |
[10]
Therefore, it is important to identify predictors of stroke recurrence after the first AIS in children. It is important to educate the parent regarding the risk of stroke recurrence in this patient. Long-term follow-up may be needed in this patient to ensure early detection of recurrence stroke, especially in the first three years after the first event.